
Menu
Refer to section 15.03 (page 134) in the BCCOHP Bylaws for more information about marketing standards.
The Boundaries in the Practitioner-Patient Relationship guideline document considers the question of when it is appropriate to enter into a practitioner-patient relationship and sets out the ethical obligation of registrants to ensure the treatment is appropriate.
The document provides guidance to registrants to help recognize conflicts and gives advice on how to resolve these conflicts.
Documentation
 Boundaries in the Practitioner-Patient Relationship Guideline
Boundaries in the Practitioner-Patient Relationship Guideline
We recognize that this is a complex and nuanced topic. To help registrants better understand how the guideline applies to them, we have produced a video.
Key Points
There are three elements that must be in place before providing treatment to any patient:
These principles are enshrined in legacy College of Dental Surgeon of BC’s Code of Ethics. They may be compromised when treating anyone with whom there is such a close personal relationship as to create a conflict of interest.
Practitioners should exercise care and judgment in:
The Clinical Practice Guideline for the Early Detection of Oral Cancer provides guidance about the appropriate use of oral cancer screening techniques to help dentists make informed decisions about screening for oral cancer. It was developed by the BC Oral Cancer Prevention Program of the BC Cancer Agency in partnership with the legacy College of Dental Surgeons of BC.
Documentation
Clinical Practice Guideline for the Early Detection of Oral Cancer
Key points
The purpose of this guideline is to:
Radiographs* (X-rays) are necessary for the evaluation and diagnosis of many oral conditions and diseases. The Dental Radiography Standards & Guidelines were approved and published in September 2015, and articulate the legacy College of Dental Surgeons of BC’s expectations for registrants regarding dental radiation (including the use of cone beam computed tomography (CBCT) in dentistry).
*For the purpose of this document radiographs includes images
Documentation
Dental Radiography Standards & Guidelines
Key Points
Good dental recordkeeping is critical to the practice of dentistry. It ensures continuity of care for patients and may help to reduce the likelihood of a complaint. The Dental Recordkeeping Guidelines contain the requirements for dental recordkeeping and the ownership, transfer and retention of dental records.
Documentation
Dental Recordkeeping Guidelines
Sample charts/forms
Key points
Dentists must now maintain complete patient records as follows:
In addition to clinical records, other records that must be retained include appointment records, lab prescriptions and invoices. Diagnostic or study models are also considered part of the permanent patient record and must be kept for the prescribed period.
Working models do not have to be retained for any specific period of time. A decision to keep working models should be based on the complexity of the case and is left to the judgment of the individual practitioner.
Exceptions: The above guidelines do not apply to minors and person under a disability. In these cases, the limitation periods do not begin running until the person turns 19 or until the disability ends.
Since the Standards and Guidelines for Minimal and Moderate Sedation was published in May 2014, the legacy College of Dental Surgeons of BC has received questions about whether or not Certified Dental Assistants are allowed to dispense medication.
In response, the legacy CDSBC CDA Advisory Committee drafted the document, Dispensing of Non-Prescription Medication by Certified Dental Assistants. This document outlines when dentists are allowed to delegate and supervise CDAs in the dispensing of medication.
Documentation
Dispensing of Non-Prescription Medications by Certified Dental Assistants
Key Points
Obstructive sleep apnea (OSA) is a medical syndrome that is characterized by recurrent episodes of partial or complete upper airway obstruction during sleep. The Obstructive Sleep Apnea Standards and Guidelines identify the roles and responsibilities of a dentist treating patients with OSA.
Documentation
Obstructive Sleep Apnea Standards and Guidelines
The purpose of the Obstructive Sleep Apnea Standards and Guidlines document is to:
Standard: A dentist’s role in the treatment of OSA is adjunctive, supplementary and/or collaborative to that provided by the physician. A dentist may provide OA therapy only after receiving a written request or prescription from the attending physician, preferably a physician with advanced training in sleep medicine. Because of the increased rates of morbidity and mortality associated with OSA, a physician (family physician or sleep specialist) must assess the potential for other medical conditions, including OSA, before a dentist provides any treatment for primary snoring.
Home Testing Equipment for Obstructive Sleep Apnea
The treatment of obstructive sleep apnea requires interdisciplinary teamwork between dentists and medical practitioners.
Dentists who rent or provide home sleep apnea testing (HSAT) equipment to patients, through limited business corporations or otherwise, are reminded that the prescription or direction for the provision of overnight home sleep testing equipment must come from a registered medical practitioner. The Ministry of Health requires that anyone doing HSAT must be accredited by the College of Physicians and Surgeons’ Diagnostic Accreditation Program (DAP).
Patient-centred care is defined as care that “is respectful of and responsive to individual patient preferences, needs, and values, and [that ensures] patient values guide all clinical decisions.”
Patient-centred Care and the Business of Dentistry is a foundational ethical document for oral health professionals. The practice of dentistry is changing and so are the economic realities of the profession. This has given rise to new business models that are challenging the traditional ways dentistry has operated. Even as the profession evolves, what cannot change is the focus on the patient.
Documentation
Patient-centred Care and the Business of Dentistry
Key points
This document addresses the inherent ethical challenges of the dual role of a dentist as a treating healthcare professional and as a business person, and holds them up against the patient’s perspective.
It includes 11 principles that reinforce patient-centred care – the principles articulate the conduct expected of registrants, reinforce owners’/managers’ accountability for the conduct of their practices, and are broad enough to apply to all practice arrangements. They are intended to supplement, not subsume, the Health Professions Act and legacy College of Dental Surgeons of BC’s Code of Ethics.
The College is frequently asked about the use of prescription drugs in dentistry. Dentists with a full, academic or restricted to specialty registration can prescribe drugs under the Health Professions Act. Dentists may need to administer drugs to provide treatment to a patient or a written prescription may be indicated afterwards. Therefore, it is essential that dental professionals know the requirements for prescribing and dispensing drugs.
The purpose of these standards is to assist registrants in regards to dispensing and prescribing drugs to ensure the safe and effective use of prescription medication.
Documentation
Prescribing and Dispensing Drugs Standards and Guidelines
The Controlled Prescription Program sets the requirements for prescribing controlled substances and was established to prevent forgeries and reduce inappropriate prescribing of selected drugs.
Duplicate prescription pads
Order a duplicate prescription pad >>
Dentists who wish to prescribe any of the monitored drugs must order their duplicate prescription pads through BCCOHP. Dentists without these pads cannot prescribe the monitored drugs. Prescription pads are personalized and numerically recorded, the prescription pad must be maintained intact in chronological order. Some practitioners may require multiple pads due to the nature of their practice, if so, you must advise BCCOHP in writing.
Dentists practising as a locum in more than one office are not required to have their practice address imprinted on the prescription scripts; however, your name and BCCOHP registration number must be imprinted. Only when you are writing the prescription must you then add the practice address and phone number of the practice where the prescription is being written.
Returning prescription pads
Dentists must return all partially and fully unused prescription pads to BCCOHP offices (by XpressPost or courier) for shredding if any of the following occur:
Lost or stolen prescription pads
In the case of lost, stolen or forged prescription pads registrants must:
Learn more about lost or stolen prescription pads >>
Additional prescription information
Resources
Wellness program The wellness program (see Health Matters section on this page) assists dentists, dental therapists or CDAs who are facing addiction or any health issues that could affect their ability to provide safe patient care. Questions about the wellness program? |
The following interpretive guidance is applicable to both the dental office setting – whether or not the dentist is on site – and to private dental hygiene practice.
On February 24, 2020, the Ministry of Health announced amendments to the regulations (scope of practice statements) for dental hygienists, dental technicians, denturists and dentists. Two of the changes that affect the provision of dental hygiene services are:
|
|---|
It is expected the decision to administer a Schedule I drug will be based on collaborative discussion and decision-making amongst the patient, dental hygienist and dentist and include thorough documentation of those discussions and decisions, including the authorization by the dentist to dispense the drug.
In order for a patient to provide informed consent for the administration of a Schedule I drug, it is expected that patient will be made aware of all of the risks, benefits, associated costs and options (including not administering the drug). In the case of anaesthetic containing a vasoconstrictor, this would include a discussion that while this formulation increases the depth and duration of anaesthesia, it may impact cardiac function.
The dental hygienist and dentist must be satisfied that, following a thorough clinical assessment and review of the medical history, there are no contraindications to the administration of the Schedule I drug.
A prescription can be defined as an authorization for the dispensing of a drug to a patient and may be written or verbal.
Within the traditional model of a dental hygienist and dentist working collaboratively within the same office, the specific requirement in the amended regulations of a prescription prior to administration of a Schedule I drug by a dental hygienist is not expected to change existing protocols. Rather, it will serve to focus the entire dental team on the existing standards of collaborative care, including a complete pre-treatment assessment of the patient, reviewing and updating of the patient’s medical history and a determination through discussion between the dental hygienist and dentist of the need for the administration of the drug for the patient.
Once a need is determined, the dentist can provide a verbal authorization for the drug to be dispensed to the patient and the dental hygienist can proceed with the administration, regardless of whether the dentist is on site or not.
In the case of a private dental hygiene practice, the authorization can be provided by a written prescription from the dentist for the patient or over the phone following the expected standards of collaborative care including assessment, review, and thorough discussion between the dental hygienist and the dentist.
A dentist may choose to make a standing order prescription for a given patient to cover a specific time frame (e.g. three to six months). If this is the case, it is expected the hygienist will review, update and document the patient’s medical status as well as revisit and determine the ongoing need for the drug before each subsequent administration, engaging the prescribing dentist in discussion should any changes be noted.
It is expected the patient record will include:
Reference documents |
|---|
|
All general dentists and certified specialists administering sedation and general anesthesia must adhere to the requirements outlined in BCCOHP’s relevant standards and guidelines.
Keep up to date on sedation and GA news here >>
Documentation
Standards & Guidelines | Addenda |
|---|---|
|
|
|
|
|
|
Register your sedation qualifications / apply for facility authorization
General dentists and certified specialists who intend to provide moderate sedation, deep sedation or general anesthesia must have their qualifications approved by BCCOHP.
Facilities where deep sedation and/or general anesthesia will be administered must first be inspected and authorized.
Questions?
Learn more about sedation and anesthesia here. If you have questions, please contact us.
The Infection Prevention and Control Guidelines provide oral health care providers with the knowledge of principles and standards to inform and properly implement necessary infection prevention and control measures in a safe and effective manner.
The legacy College of Dental Surgeons of BC’s Board approved the Infection Prevention and Control Guidelines at its May 2012 meeting, and the document was distributed to dentists and CDAs with the summer 2012 Sentinel.
Documentation
The following standards describe the responsibilities of dentists, dental therapists and certified dental assistants (CDAs) in providing dental care to the public in B.C.
The purpose of this information sheet is to identify when it is within the Dentists Scope of Practice to prescribe and administer Schedule 1 medications, such as Botulinum Toxin Type A (i.e. Botox®) and smoking cessation drugs, such as Zyban®.
Documentation
Key Points
– the patient is a “patient of record” at the dental practice;
– the drug is part of a comprehensive dental treatment plan;
– the patient has received a comprehensive dental examination;
– the patient completed a full medical history and has been assessed;
– informed consent has been obtained;
– treatment takes place in an appropriate clinical setting.
The ”Use of dermal fillers remains outside the scope of practice of dentists” document that was previously ported over to BCCOHP from College of Dental Surgeons of BC was removed on April 5, 2024 as it was determined that it does not align with BCCOHP’s regulations and bylaws.
The core of the dentist-patient relationship is a trusting relationship. This document provides some of the key obligations and roles that each of the dentist and the patient can expect of each other.
With a better common understanding of what can be expected from each party, communication between dentists and patients can be improved, and concerns that could mature into a complaint can be resolved quickly and amicably between the doctor and the patient.
Documentation
The purpose of this information sheet is to provide clarity to registrants and the public about the issue of settlement agreements and complaints to the College.
Documentation
Key Points
The purpose of this information sheet is to outline the appropriate process for dismissing a patient when the dentist-patient relationship breaks down and cannot be repaired.
Documentation
Dismissing a Patient – Practical and Ethical Concerns
Key Points
The purpose of this information sheet is to provide clarity to registrants and the public regarding the use of VELscope screening to identify potential oral mucosal diseases, including oral cancer.
Documentation
Key Points
As of June 1, dentists in BC can become authorized to access PharmaNet. This joint initiative between legacy CDSBC and BC’s Ministry of Health marks a significant and positive change that will enhance the safety of dental patients and the public.
Practitioner access to PharmaNet is only for the purpose of direct patient care: providing health services to an individual in the context of a professional health practice. It is subject to strict privacy and security measures designed to prevent unauthorized access and protect the information of BC residents.
As a prescribing dentist, you may permit other regulated oral health professionals to use PharmaNet on your behalf, specifically and directly to support clinical care (e.g., to populate a patient’s chart before a visit).
What is PharmaNet?
PharmaNet is the province-wide network that links BC community pharmacies to a central data system. It keeps a record of every prescription dispensed in a BC community pharmacy and is administered by the Ministry of Health. PharmaNet:
Who can access PharmaNet?
June 1, 2022 is the beginning of the enrollment period for dentists (independent PharmaNet users) and those they designate to support them (on-behalf-of users).
There are five steps you must complete in order to apply for access to PharmaNet. More information about each is below, together with links to relevant resources.
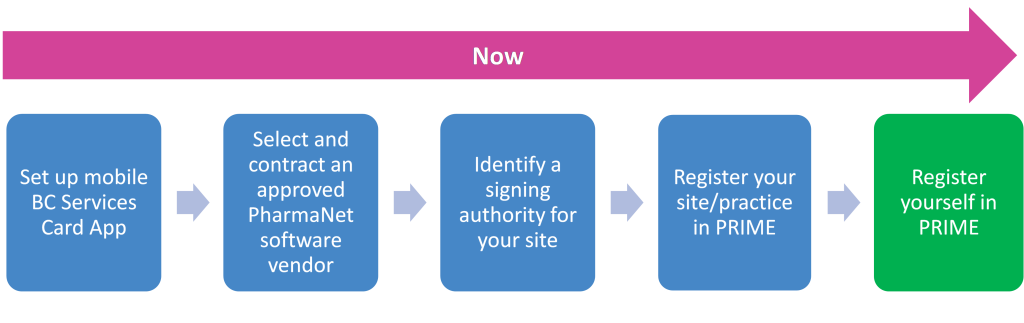
Step 1: Set up your mobile BC Services Card app
If you do not already have the BC Services Card on your mobile device you will need to set it up.
Note: The BC Services Card app connects with PRIME – the system used to connect health care providers with PharmaNet. PRIME uses your name, birthdate and address from the BC Services Card.
Set up your mobile BC Services Card
Step 2: Choose a vendor
Next, research and contract an approved PharmaNet software vendor. Below is a list of vendors who have confirmed their ability to work with dentist PharmaNet users:
Please note: although PharmaNet lists five software vendors on its web page, only two have confirmed that they can provide this service for registrants.
Step 3: Identify a signing authority
Identify a signing authority. This person, or someone they delegate to, will register the site in PRIME (see step 4). The signing authority will need:
Step 4: Register your site/practice in PRIME
The signing authority, or delegate, must register the site/practice in PRIME.
A “site” is a combination of the practice’s physical location and PharmaNet software vendor. If a practice uses the PharmaNet application of more than one vendor, it has more than one site; each must be registered separately, but under the same responsible organization.
If you have completed steps 1-3, follow the instructions in the online video tutorial to register your site in PRIME.
Step 5: Register yourself in PRIME
You will need:
Note: You will not receive a confirmation email. You can log in to PRIME to check your status.
If you have already enrolled in PRIME
Dentists are independent PharmaNet users as of June 1, 2022.
If you enrolled in PRIME before June 1, 2022 as a Dentist you need to:
Visit PRIME for more information and a how-to video, or begin your enrollment through the PRIME application.
Resources
Support
BC Services Card App Support
1-888-356-2741 (Canada and USA toll free)
604-660-2355 (Within Lower Mainland or outside Canada and USA)
PRIME Support
1-844-397-7463
PRIMESupport@gov.bc.ca
